
Behind an apparently simple and thankfully, non-fatal crash landing, lay a complex brew of errors, factors and assumptions.
On 19 December 2019, a turbine powered Cessna P210N took off from Bankstown Airport, in Sydney, for a private IFR flight to Cambridge Airport, near Hobart. A pilot and a passenger were on board. They had the very best of general aviation to look forward to: a fast smooth journey in the flight levels, breathing heated pressurised air, high above the smoke and turbulence that bushfires were creating over south-eastern Australia in that disastrous month.
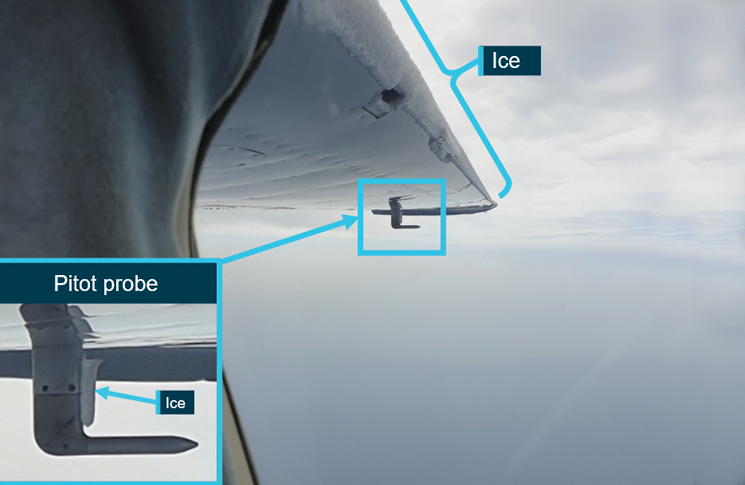
Shortly after reaching cruise altitude of about 18,000 feet, the US-registered Cessna encountered icing conditions. The pilot requested and was granted ATC clearance to descend to 16,000 feet. During this descent, the pilot turned off the propeller de-ice and engine ice-protection systems. Another engine ice-protection system, which functioned automatically when the aircraft was pressurised, continued to operate. At 16,000 feet, the pilot made several track deviations to avoid entering cloud. The pilot also took several photographs, including one which showed ice on the leading edge of the left wing and pitot probe.
Then the engine stopped. The pilot reacted swiftly, attempting a restart within 5 seconds of shutdown. This was unsuccessful and the pilot declared mayday and was directed to Moruya airport.
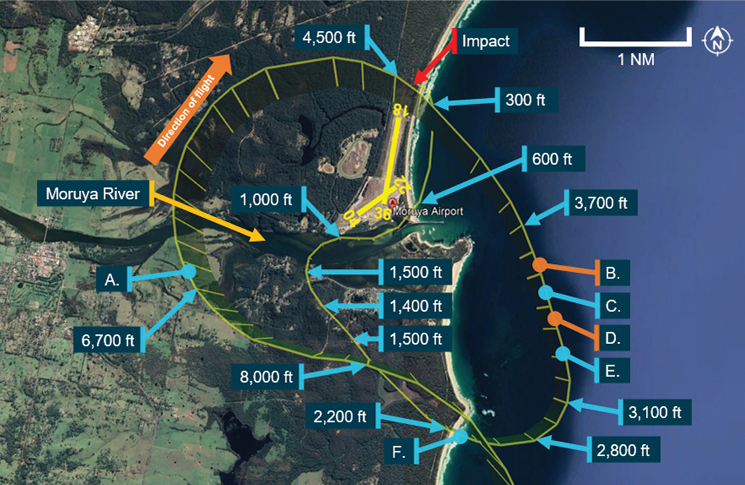
The pilot found the aircraft behaved differently in a real glide to the way it had handled during simulated glide training earlier that year in the US. In a real emergency the aircraft glided better, losing less altitude. The Cessna arrived at Moruya from the south at 8,000 feet, circled to approach runway 18 but was too high. Smoke haze obscured the runway even though it was only 2 nm away. The pilot put down the landing gear and at least 10 degrees of flap, at about 6,000 feet, to lose altitude. This was much higher than would normally be done in a glide approach. About the same time the pilot’s attention began to be dominated by a shark patrol Robinson R44 helicopter in the vicinity.
The pilot found the aircraft behaved differently in a real glide to the way it had handled during simulated glide training.
The R44 pilot flew directly to the airport, intending to land and avoid distracting the Cessna pilot but modified this plan, instead hovering offshore at 200 feet abeam the midpoint of the main runway.
The Cessna pilot continued the orbit but, after encountering turbulence and windshear, was now too low for another attempt at runway 18.
Unable to see the runway, uncertain about the position of the helicopter and unstabilised by windshear with the aircraft in a high-drag configuration, the Cessna pilot was running out of options. The pilot rejected landing on runway 36 or runway 22 and continued to fly north for a second attempt at runway 18. Abeam the threshold of runway 18, at 300 feet, the pilot realised a landing was unlikely and continued northward, slowing and instructing the passenger to tighten their seat belt. The aircraft struck trees and crashed 560 metres north of the airport just under an hour after taking off.
Instant response
From a vantage point over the sea, the R44 pilot saw the crash and flew at once to the site where the observer jumped out from a low hover and helped the people in the Cessna. Defence Force paramedics had been taking part in a skydiving exercise at Moruya airport and were already heading to the crash site by car. The R44 pilot guided them to the accident site from the air before landing nearby. The skydive instructors and R44 observer attempted to remove the unconscious pilot from the aircraft but could not open the main entry door. A paramedic helped the injured passenger who had crawled through the broken front windscreen. Fuel was leaking from the aircraft, so the chief skydive instructor reached through the broken windscreen and switched off its electrical systems. The rescuers used a tyre lever to pry open the aircraft door and rescue the seriously injured pilot. The passenger had minor injuries.
Common sense confounded
Like most aircraft accidents and incidents, the crash was the result of a convergence of factors. And like most aircraft accidents, these factors are much more easily seen in hindsight than before the event.
The pilot’s decision to switch off continuous ignition and compressor inlet heat had contributed to ice build-up which probably silenced the engine when it was ingested, the Australian Transport Safety Bureau (ATSB) found.
The pilot, who had 430 hours, including 162 in a P210N, told ATSB investigators, ‘If you get into inadvertent icing, get out of it’, a concise and common sense maxim. Commonsense had also guided him to switch off the ice-protection systems once the aircraft was no longer in visible moisture and not accruing any more ice. But in this case, common sense was at odds with the flight manual, which said, ‘These systems must be operated in the above mentioned conditions (snow or temperature below 5 degrees) even if there is no visible sign or airframe ice and/or snow accumulation.’
The pilot’s promptness in attempting to restart the engine was because of an awareness of rotor lock, a temporary seizure of the engine caused when the cooling generator case contracts around the hot generator turbine. The engine’s maker, Rolls-Royce, was unable to say whether rotor lock had definitely occurred. The company’s engineers said they would have expected to see more signs of turbine blade rub along the first or second stage gas producer turbine blade track than the ATSB’s teardown found, and that attempting to start a fully locked engine would have tripped the starter/generator circuit breaker – which did not happen.
The ATSB concluded rotor lock caused by ice ingestion was the most likely reason the engine had stopped. Only 30 g of ingested ice would stop an engine, a Rolls-Royce study had found. And while in theory the engine could have been restarted in the warmer air below 6,000 feet, the ATSB found this would have been unreasonable to expect while the pilot was late in a glide approach.
How the pilot had inadvertently encountered icing was another factor. The pilot had been using a US electronic flight bag (EFB) service, Foreflight, which was not approved by CASA. Moreover, outside the US, Foreflight only offered a more basic version of its service, which did not include AIRMETs (advice on deteriorating conditions not already included in the relevant area forecast) and SIGWX (significant weather) charts covering FL 100–FL 250 for Australia. Foreflight’s website mentioned this but the forecast did not and the pilot assumed all relevant weather information was being provided as it would have been in the US and Europe. This meant an Australian Bureau of Meteorology SIGWX chart indicating moderate icing above 10,000 feet went unseen by the pilot.
Also, Foreflight did not alert the pilot to the aircraft being 50 kg over maximum take-off weight; however, this was not judged to be a contributing factor to the accident. And the Foreflight checklists the pilot used had several important omissions: to isolate the engine from the fuel supply for a forced landing, warn about rotor lock and secure shoulder harnesses (although the pilot had the common sense to address 2 of these things, unprompted).
Deploying electrically powered landing gear and flaps before power is lost might seem like common sense, but the more refined common sense of aviation, derived from decades of often bitter experience, says, ‘Never add drag or reduce lift from an unpowered aircraft until your landing is assured.’
In the final phase of the flight, the pilot had focused on slowing the aircraft to 44 knots, based on a belief that it was the aircraft’s stall speed. The stall speed for a Cessna P210N is 59 knots
The ATSB concluded that the pilot’s focus on the R44 helicopter had caused a distraction from managing the aircraft’s speed, position and altitude, and caused the pilot to misjudge an approach to the remaining viable runways (runways 36 and 22).
Imagine what that silence after prop winddown would have been like, with life or death decisions to be made.
‘This misjudgement resulted in the aircraft arriving at a position where an offairport landing was the only option, leading to the collision with terrain,’ the ATSB said.
The pilot had said much the same in different terms on an aviation forum. ‘I probably should have told the local traffic to bugger off and put her down on 18 on the first circuit, but hindsight only works after the event.’
Two other P210N flameouts mentioned in the ATSB report had been fatal accidents but the instant presence of rescuers, luck and perhaps a moment of skill by the pilot in the final seconds produced a better outcome. The pilot, who suffered broken bones wrote on the forum, ‘I will happily take the final result any day of the week.’
Common sense proved to be no substitute for thorough knowledge and practice that a relatively inexperienced pilot flying a relatively complex aircraft lacked. Smoke haze and turbulence on the day of the crash stacked the deck further against a successful landing.
But do not judge. Instead, imagine what that silence after prop winddown would have been like, with life or death decisions to be made, while dredging procedures and numbers from the depths of memory. Now ask yourself, ‘Would I have done any better?’
Be prepared to justify your answer if it’s ‘yes’. If your answer is ‘no’ or ‘I don’t know,’ that’s good news – you get a free warning. Unlike the accident pilot you have time to study (and practice) for a better result. Aircraft systems, checklists, weather information, emergency procedures: better to hit the books than hit the ground.



